Astrocytic Hamartoma – April 2018

13-year-old boy was referred to Illinois Retina Associates for suspicion for a choroidal nevus. He had no complaints.
Past Medical History
He had a history of hypertension due to underlying polycystic kidney disease.
Medications
He was on medications for hypertension
Ocular Examination
-
Vision was 20/25 both eyes - Pressures were 10 and 12
- Pupils were equal and reactive without relative afferent pupillary defect
- The anterior segments were unremarkable
- The posterior segment photos are shown below (Figure 1). No additional pathology was seen in either periphery
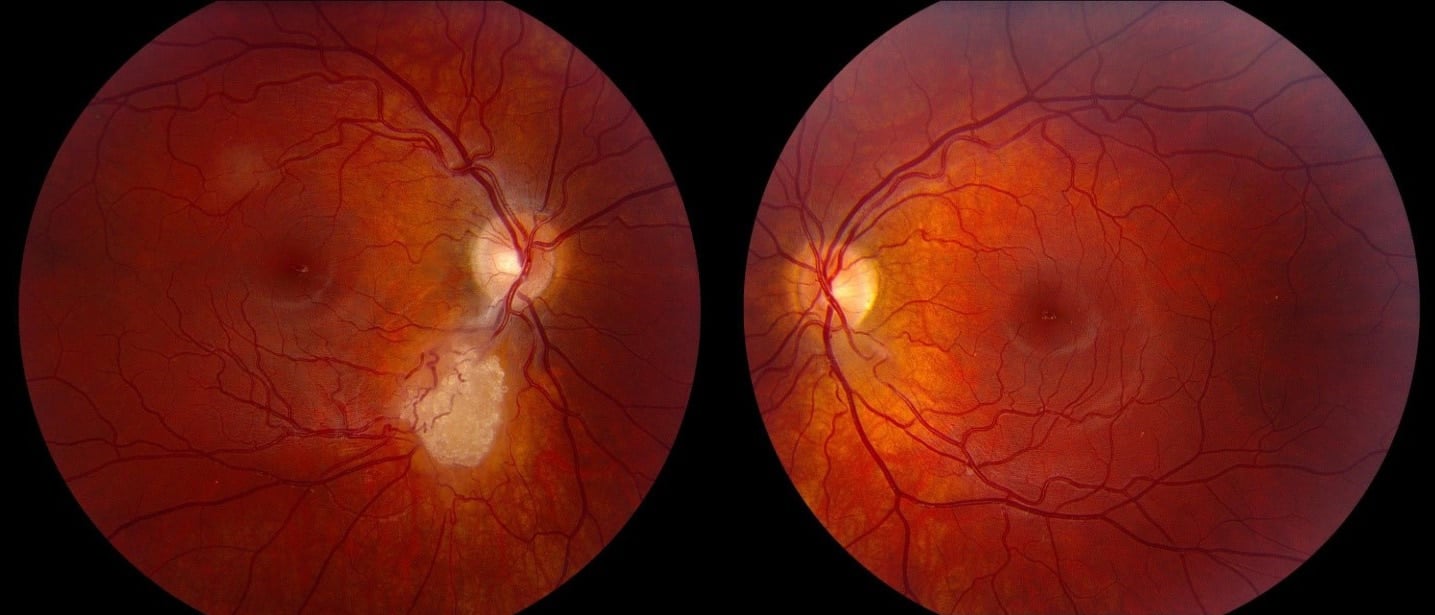
Figure 1: Posterior segment photographs
Differential Diagnosis
-
Astrocytic Harmartoma - Retinoblastoma
- Myelinated Nerve Fiber Layer
- Amelanotic Melanoma
- Choroidal Neovascularization
Further Workup
Upon questioning, the young man endorsed that he did have 6 unusual patches on his skin, which were confirmed to be consistent with ash-leaf spots.
Diagnosis
Astrocytic hamartoma of the retina due to underlying tuberous sclerosis.
Discussion
Tuberous sclerosis is a systemic disorder that can result in non-cancerous lesions in multiple organ systems. Over 90% of affected patients will have skin lesions, neurological symptoms and kidney problems. This autosomal dominant condition is believed to affect 1 in 6,000 people. The diagnosis is made based on the patient having to major, or one major and two minor features (listed below).
Major Features
-
Facial angiofibromas or forehead plaque pits in dental enamel - Non-traumatic ungula or periungual fibroma
- Hypomelanotic macules (three or more)
- Shagreen patch (connective tissue nevus) migration lines
- Multiple retinal nodular hamartomas
- Cortical tuber
- Subependymal nodule
- Cardiac rhabdomyoma, single or multiple
- Lymphangiomyomatosis, renal angiomyolipoma, or both
Minor Features
-
Multiple, randomly distributed - Hamartomatous rectal polyps
- Bone cysts
- Cerebral white matter radial
- Gingival fibromas
- Non-renal hamartoma
- Retinal achromic patch
- Confetti-like skin lesions
- Multiple renal cysts
Approximately 45% of patients with tuberous sclerosis have retinal astrocytic hamartomas. Most will maintain a stable size and will not cause visual problems. However, a minority may have a symptomatic increase in lesion size, which may be slowed or reversed with oral sirolimus. Even without an increase in size, some astrocytic hamartomas are associated with retinal bleeding or edema which may be responsive to anti-VEGF intravitreal injections.
References
Curatolo, P., R. Bombardieri, and S. Jozwiak. “Tuberous Sclerosis.” Lancet (London, England) 372.9639 (2008): 657-68. Print.
Lonngi, M., A. S. Gold, and T. G. Murray. “Combined Bevacizumab and Triamcinolone Acetonide Injections for Macular Edema in a Patient with Astrocytic Hamartomas and Tuberous Sclerosis.” Ophthalmic surgery, lasers & imaging retina 44.1 (2013): 85-90. Print.
Shepherd, C. W., et al. “Tuberous Sclerosis Complex in Olmsted County, Minnesota, 1950-1989.” Archives of Neurology 48.4 (1991): 400-1. Print.
Zhang, Z. Q., et al. “Sirolimus for Retinal Astrocytic Hamartoma Associated with Tuberous Sclerosis Complex.” Ophthalmology 122.9 (2015): 1947-9. Print.