Hydroxychloroquine Toxicity – June, 2025

History:
A 55-year-old patient with past medical history of lupus and diabetes presented to our clinic due to vision loss in both eyes (OU) worse at night for an unknown amount of time.
Exam:
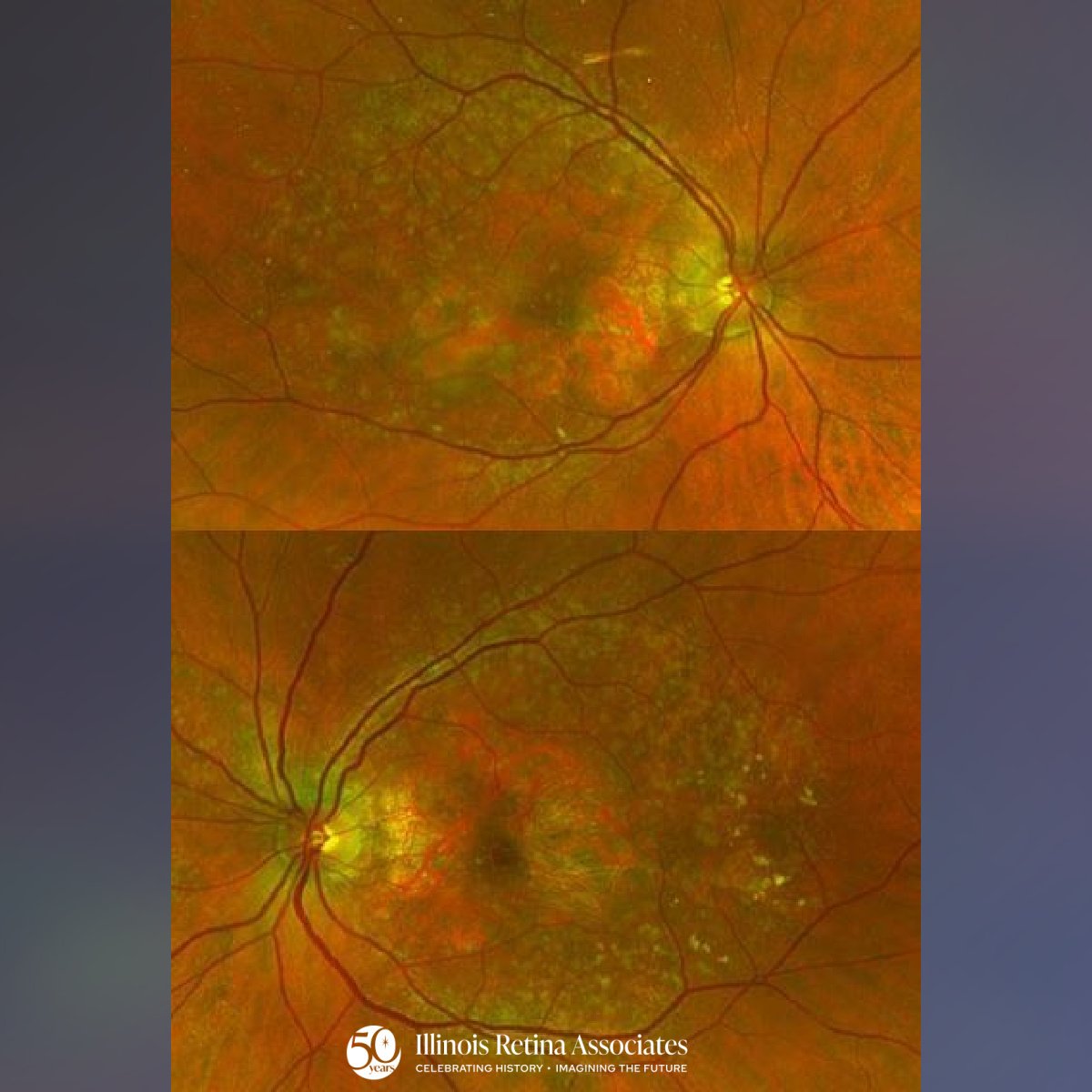
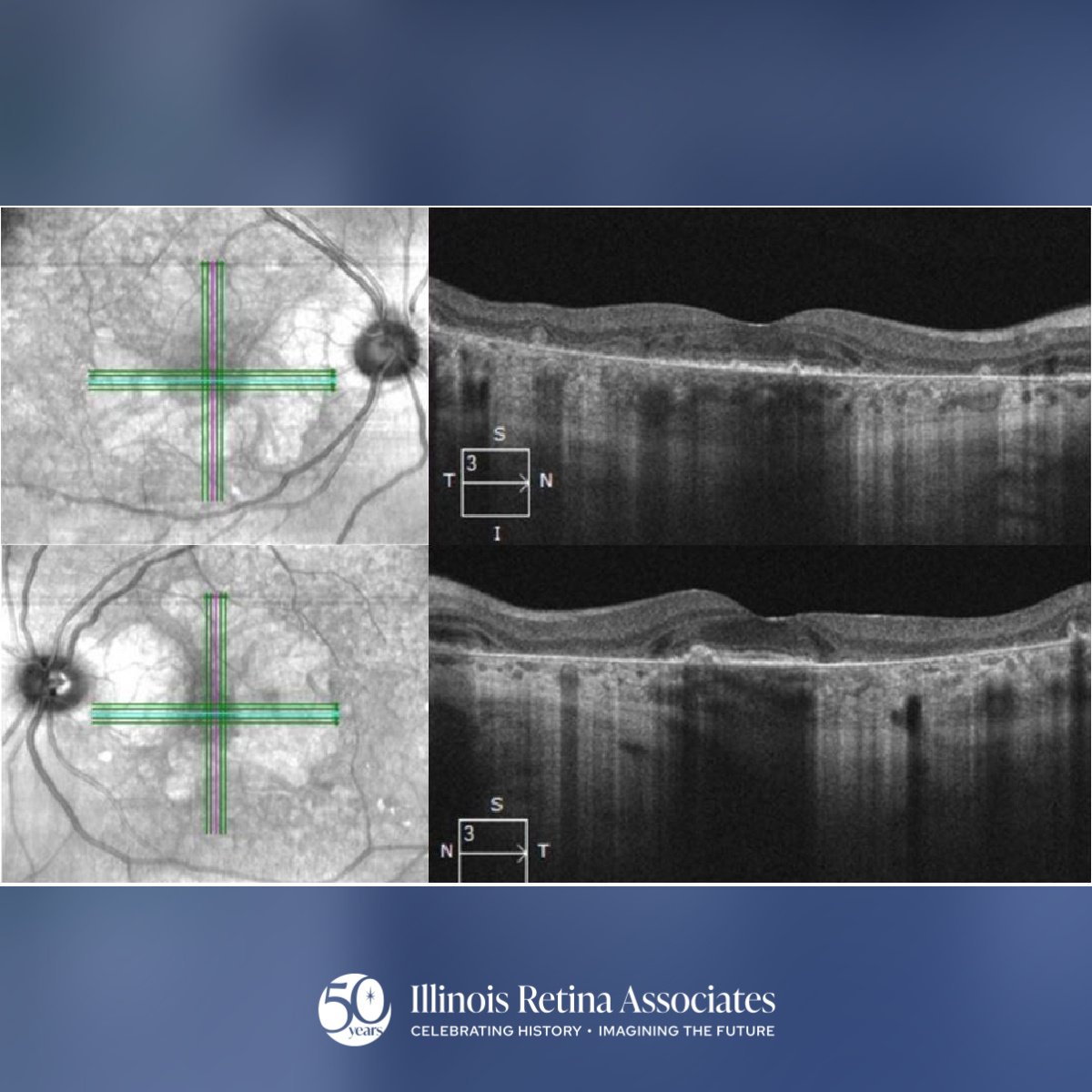
Visual acuity was 20/30 in the right eye (OD) and 20/25 in the left eye (OS). Intraocular pressure was normal, confrontation visual field was full, and anterior segment examination was notable for mild nuclear sclerotic cataract OU. Posterior segment showed 0.2 CDR, posterior vitreous detachment, and normal periphery. The macula showed parafoveal retinal pigment epithelial changes with geographic atrophy and small drusen (Fig 1). Optical Coherence Tomography (OCT) showed parafoveal outer retinal atrophy OU (Fig 2).
Differential Diagnosis:
• Advanced age-related macular degeneration
• Hydroxychloroquine toxicity
• Cone or Cone-rod retinal dystrophy
• Stargardt disease
Discussion:
Hydroxychloroquine Toxicity
The patient had a history of hydroxychloroquine use and was diagnosed with hydroxychloroquine toxicity. Given the history of lupus, the patient was on hydroxychloroquine for 25 years at 400mg daily.
Hydroxychloroquine, or Plaquenil, can cause bilateral photoreceptor destruction in a “bull’s-eye” pattern with a spared foveal island due to accumulation of the drug in the RPE resulting in cellular atrophy.1,2 The typical OCT finding is parafoveal ellipsoid zone loss with a spared central island known as “flying saucer sign”. Fundus autofluorescence may reveal early parafoveal hyperautofluorescence which may precede OCT findings.3 A baseline exam, visual field, and OCT should be completed prior to drug initiation with annual screening. Those at higher risk include patients dosed greater than 5mg/kg/day, more than 5 years of use, concomitant tamoxifen use, impaired renal function, and pre-existing macular pathology. Once retinal toxicity is suspected or recognized, efforts to discontinue the medication should be made. Unfortunately, retinal atrophy can progress for a period of time despite discontinuation of the medication. There is no treatment for regaining vision so efforts are focused on screening and early recognition.
If you are looking to schedule your first consultation, please contact us today by clicking HERE and find the location that is nearest you!
References:
- Yam JC, Kwok AK. Ocular toxicity of hydroxychloroquine. Hong Kong Med J. 2006;12:294-304.
- Marmor MF, Kellner U, Lai TYY, Melles RB, Mieler WF; American Academy of Ophthalmology. Recommendations on screening for chloroquine and hydroxychloroquine retinopathy. Ophthalmology. 2016;123:1386-1394.
- Marmor MF. Comparison of screening procedures in hydroxychloroquine toxicity. Arch Ophthalmol. 2012;130:461-469.