Acute Idiopathic Maculopathy – December, 2025

History:
A 41-year-old female was referred for blurry vision in the left eye for 1 week. She denied any viral prodrome, floaters, flashes, or curtain over vision.
Exam:
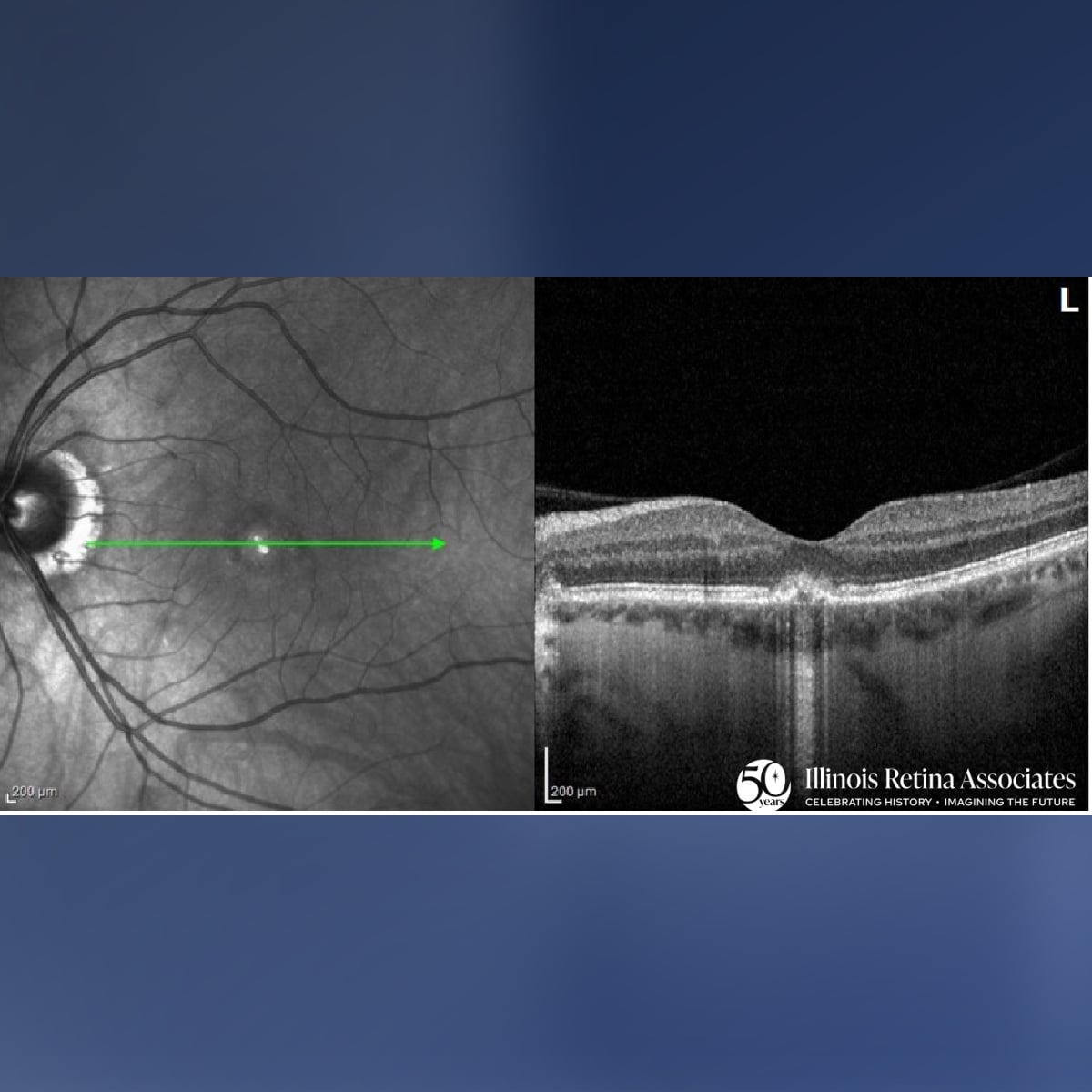
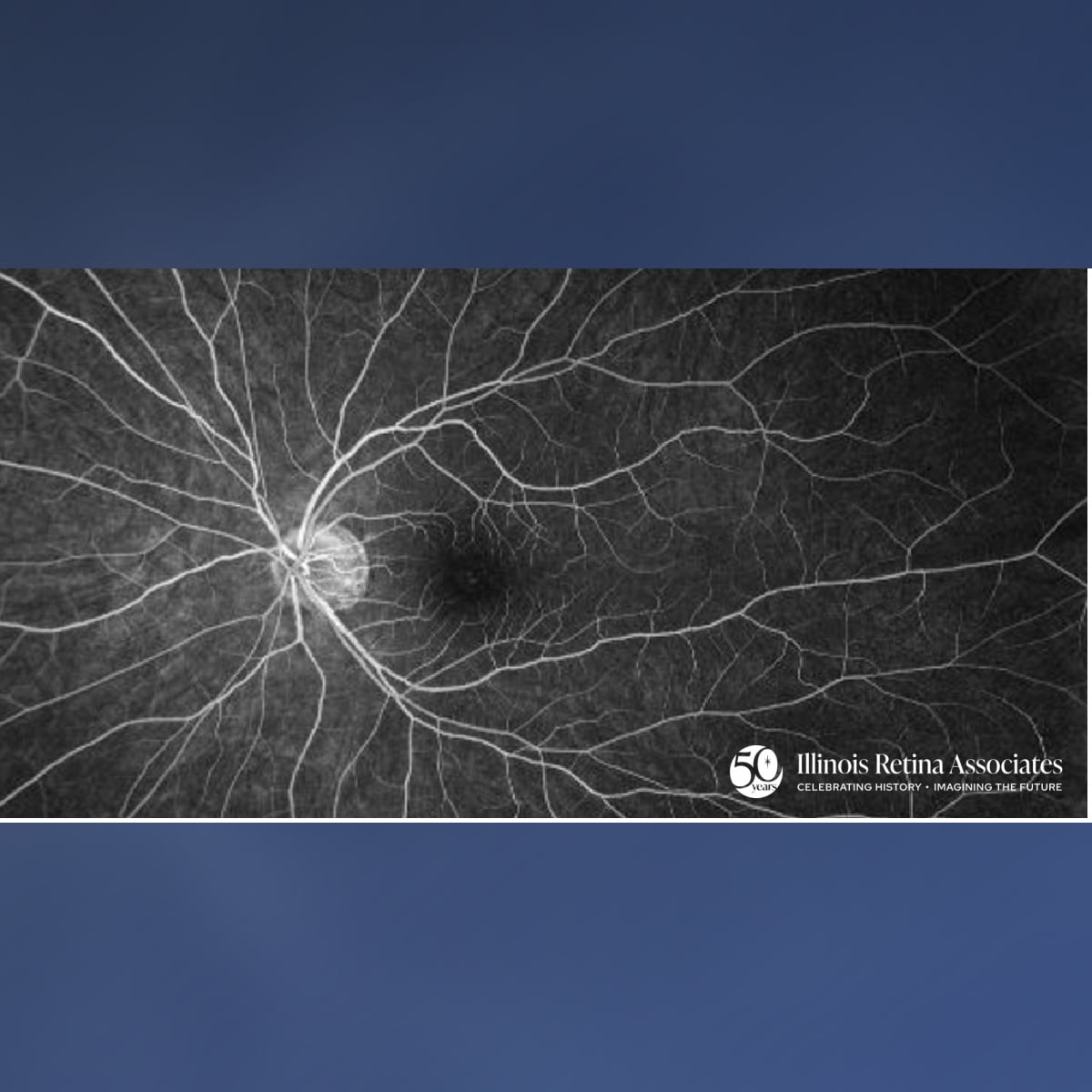
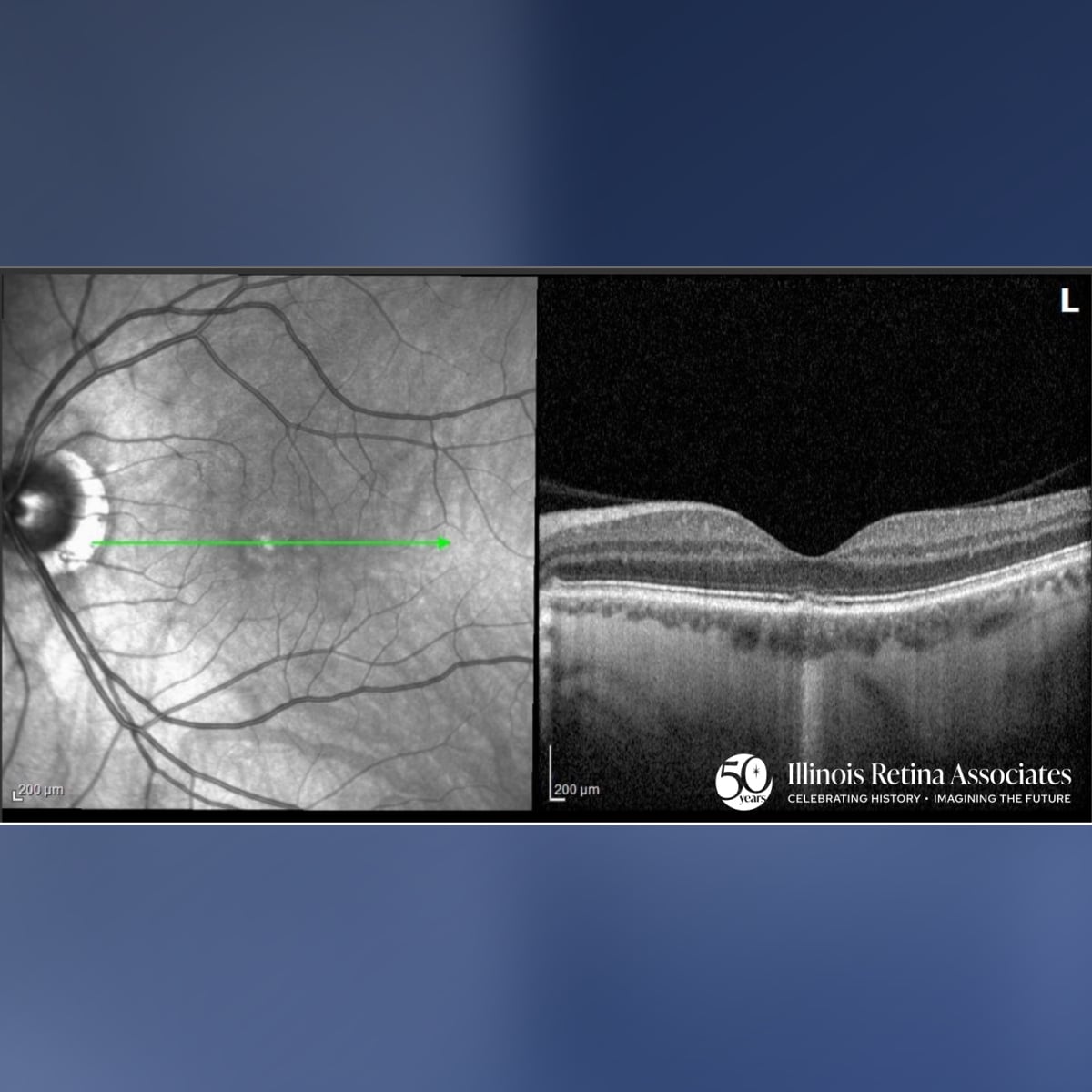
Visual acuity was 20/20 in the right eye (OD) and 20/80 in the left eye (OS). Intraocular pressures were normal in both eyes (OU) and anterior segment exam was normal OU. Posterior segment exam and Ocular Coherence Topography (OCT) OD were unremarkable. Posterior segment exam OS revealed a normal cup, peripapillary atrophy, and central RPE changes (Fig 1) and OCT was significant for irregularity the outer retina and RPE with ellipsoid zone disruption (Fig 2). Fluorescein angiography was normal OD and significant for staining of the RPE changes OS (Fig 3). OCT-A did not suggest presence of CNVM OS. Fundus autofluorescence demonstrated mild central hypo-autofluorescence. The patient was followed over 2 months during which her VA improved to 20/30, and OCT demonstrated ellipsoid zone reconstitution (Fig 4).

Differential Diagnosis:
- Acute Idiopathic Maculopathy
- Central Serous Chorioretinopathy
- Acute Posterior Multifocal Placoid Pigment Epitheliopathy
- Punctate Inner Choroidopathy
- Harada Syndrome
Discussion:
Acute Idiopathic Maculopathy
Acute idiopathic maculopathy is a rare, self-limiting inflammatory disease of the macula that typically causes sudden, unilateral, and painless central vision loss in otherwise healthy young adults. VA can be reduced to 20/200 or worse at presentation and can be preceded by a flu-like illness which has been associated in some cases with coxsackievirus infection.1,2 Diagnosis is made clinically with patient history, exam, and imaging. Exam findings may include RPE changes, foveal/parafoveal thickening, serous macular detachment, and CME. OCT can be used to diagnose photoreceptor outer segment disruption and FA, FAF, and OCT-A can be used to assess for RPE abnormalities and presence of subretinal fluid or CNVM.3 Vision often recovers spontaneously over days to weeks, with most patients regaining near-normal acuity.4
If you are looking to schedule your first consultation, please contact us today by clicking HERE and find the location that is nearest you!
References:
- Fuente, Miguel A. De La, and Rubén Cuadrado. "Unilateral Acute Idiopathic Maculopathy: Angiography, Optical Coherence Tomography and Microperimetry Findings." Journal of Ophthalmic Inflammation and Infection. Springer-Verlag, 24 Nov. 2010. Web. 26 Nov. 2016.
- Yannuzzi LA, Jampol LM, Rabb MF, Sorenson JA, Beyrer C, Wilcox LM., Jr Unilateral acute idiopathic maculopathy. Arch Ophthalmol. 1991;109:1411–1416. [PubMed]
- Nicolo M, Rosa R, Musetti D, Musolino M, Traverso C. Early Swept-Source Optical Coherence Tomography Angiography Findings in Unilateral Acute Idiopathic Maculopathy. Ophthalmic Surg Lasers Imaging Retina. 2016; 47: 180-182. doi: 10.3928/23258160-20160126-13
4.. Gupta, A., S. Rogers, and B. N. Matthews. "Unilateral Acute Idiopathic Maculopathy." British Journal of Ophthalmology 93.8 (2009): 1073-074. Web.